
Phlebotomy Essentials
6th Edition
ISBN: 9781451194524
Author: Ruth McCall, Cathee M. Tankersley MT(ASCP)
Publisher: JONES+BARTLETT PUBLISHERS, INC.
expand_more
expand_more
format_list_bulleted
Related questions
Question
Questions need to be answere.
1. What's the difference between conjugated bilirubin and direct bilirubin?
2. Whe does conjugated bilirubin need to be assessed?
3. What are the clinical manifestations that would indicate development of problem/complications.

Transcribed Image Text:NEONATAL INTENSIVE CARE UNIT (NICU)
CASE STUDY NUMBER 2: Hyperbilirubinemia
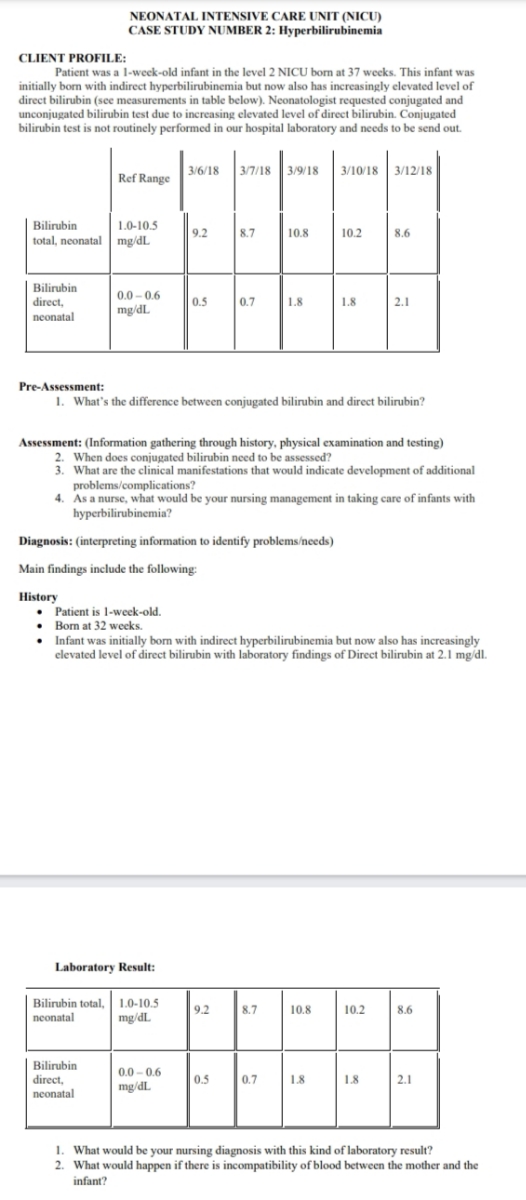
CLIENT PROFILE:
Patient was a l-week-old infant in the level 2 NICU born at 37 weeks. This infant was
initially born with indirect hyperbilirubinemia but now also has increasingly elevated level of
direct bilirubin (see measurements in table below). Neonatologist requested conjugated and
unconjugated bilirubin test due to increasing elevated level of direct bilirubin. Conjugated
bilirubin test is not routinely performed in our hospital laboratory and needs to be send out.
3/6/18
3/7/18 3/9/18 3/10/18 3/12/18
Ref Range
Bilirubin
total, neonatal mg/dL
1.0-10.5
9.2
8.7
10.8
10.2
8.6
Bilirubin
direct,
0.0 – 0.6
0.5
0.7
1.8
1.8
2.1
mg/dL
neonatal
Pre-Assessment:
1. What's the difference between conjugated bilirubin and direct bilirubin?
Assessment: (Information gathering through history, physical examination and testing)
2. When does conjugated bilirubin need to be assessed?
3. What are the clinical manifestations that would indicate development of additional
problems/complications?
4. As a nurse, what would be your nursing management in taking care of infants with
hyperbilirubinemia?
Diagnosis: (interpreting information to identify problems/needs)
Main findings include the following:
History
• Patient is 1-week-old.
• Born at 32 weeks.
Infant was initially borm with indirect hyperbilirubinemia but now also has increasingly
elevated level of direct bilirubin with laboratory findings of Direct bilirubin at 2.1 mg/dl.
Laboratory Result:
Bilirubin total, 1.0-10.5
mg/dL
9.2
8.7
10.8
10.2
8.6
neonatal
Bilirubin
direct,
neonatal
0.0 - 0.6
mg/dL
0.5
0.7
1.8
1.8
2.1
1. What would be your nursing diagnosis with this kind of laboratory result?
2. What would happen if there is incompatibility of blood between the mother and the
infant?
Expert Solution
This question has been solved!
Explore an expertly crafted, step-by-step solution for a thorough understanding of key concepts.

Step by stepSolved in 2 steps

Knowledge Booster

Similar questions
- 3:09 º coursera.org/learn/pat + ℗ Lesson 2 Quiz Back . Graded Quiz 15 min 10 total points English Due Jun 23, 11:59 PM -04 9. An example of inevitable harm is: An allergy to an appropriate drug therapy with no history of allergy Pharmacy technician makes the wrong medication for a patient Physician fails to order an X-ray when it is indicated None of the above 10. Which factor(s) should be considered when evaluating the risks of a given treatment or therapy? Complete a benefit assessment of acceptable versus unacceptable risks Patient/caregiver wishes Both of these Neither of these ||| O < 1 point 1 pointarrow_forwardWeb Assignments 1. Conduct online research on cystic fibrosis. Prepare a report on the following: ● Inheritance pattern of cystic fibrosis Diagnosis and treatment of cystic fibrosis in children Learrow_forwardAnswer questions thoroughlyarrow_forward
- 4 and 5arrow_forwardQuestion:- Case Study #1 Chapter 21: Skin and eye infections You patient is a 54-year-old female. Her height is 5’3” and weight is 396 lbs. She complains of a rash in the folds of her abdominal skin that has been getting worse over the last several weeks. She states that the rash is very red and itchy. While observing the patient you notice her fingernails are discolored and appear thickened. You also notice an odor coming from the patient. What is your diagnosis? (be specific and defend your answer using the case history) What is(are) the causative agent(s) of this diagnosis? What test would you perform to confirm your diagnosis? How might this have been prevented? What is the recommended course of treatment? If untreated, what are the risks to the patient for this diagnosis?arrow_forwardI need complete drug study for this pls help me IV lidocaine It is administered to suppress the premature ventricular contractions Therapeutic level of IV lidocaine The therapeutic level of Lidocaine should be maintained between 1.5-5.0 mcg/mL Toxic level of lidocaine is 4.5mg/kg Monitor for lidocaine toxicity such as circumoral numbness, tongue paresthesia, and dizziness Watch for tinnitus and blurred vision Note : Lidocaine dose should be administered 1 to 1.5 mg/kg Repeat with 0.5 to 0.75 mg/kg every 5 to 10 minutes as necessary (maximum cumulative dose: 3 mg/kg) Reduce the rate of infusion after the prolonged infusion (after 24hours) Constant ECG monitoring is mandatory while administering this medication.arrow_forward
- uestion 1 Match the meanings with their correct terms. low levels of blood sugar treatment of the mind study of tumors excision of the stomach pertaining to producing cancer abnormal condition (slight increase) of white blood cells brain disease abnormal condition of the skin cancerous condition of white blood cells pertaining to produced by treatment A. dermatosis B. hypoglycemia C. leukocytosis D. iatrogenic E. encephalopathy F. oncology G. gastric resection H. psychiatry I. leukemia J. carcinogenicarrow_forwardb. What is her CrCl? 4. J.C., a 70 year old male (5'8", 100 kg) is to begin Vancomycin (along with Zosyn and Levaquin) for broad-spectrum coverage for pneumonia (moderate infection with goal AUC 500-600). WBC=13.8, SCr=0.9 mg/dL. Using AUC dosing, please come up with a dosing regimen that is appropriate for JC. a. What is the dosing weight? CrCl ? b. What LD & MD & interval would you recommend? c. When should you order a vancomycin trough for J.C? Now, lets adjust his dose Assume his initial dose was 1750mg g 12h scheduled at 0900 & 2100. Assume his doses were given on time. The hospital policy required an infusion time of 2hr. The peak was 45ug/ml drawn after the 4th dose at 1230, 3.5hr after the start of the infusion. The trough level was 21ug/ml drawn at 2030, 11.5hr after the 4th dose. How would you adjust the dose? a. Calculate the patient specific k b. Calculate Cmax & Cmin c. Calculate the AUC d. Calculate patient specific Vd e. Calculate new dosing interval f. Calculate new…arrow_forwardI have case study revion question. the quesion is A 25-year-old female presented to her 28 week antenatal appointment with the complaint oflethargy. It was noted the patient appeared pale. A full blood count was taken. blood flim of pateint has been attached. so the pateints heamoglobin was low heamatcrit was low MCV was low MCH was low But RDW (RED BLOOD CELL DISTRUCTION WAS high) at 17% i have conlcuded that she has microcytic anmeia. Struggling on dicussing a diffrential diagonsis part. Give a detail diffrentianl diagnosis. and what treaments can be given.arrow_forward
- Name the correct answer!. Asap What clinical manifestation would the nurse expect to find in a client who is experiencing anaphylaxis? Dilated bronchioles, constriction of peripheral blood vessels, decreased capillary permeability. Asthma, deep vein thrombosis, encephalopathy Narrowing of the bronchioles, dilation of the peripheral blood vessels, increased capillary permeability. Left-sided heart failure, pulmonary embolism, urinary tract infection..?arrow_forwardGive written answer with explanation and conclusionarrow_forwardI need help with number 7arrow_forward
arrow_back_ios
arrow_forward_ios
Recommended textbooks for you
- Phlebotomy EssentialsNursingISBN:9781451194524Author:Ruth McCall, Cathee M. Tankersley MT(ASCP)Publisher:JONES+BARTLETT PUBLISHERS, INC.
 Gould's Pathophysiology for the Health Profession...NursingISBN:9780323414425Author:Robert J Hubert BSPublisher:Saunders
Gould's Pathophysiology for the Health Profession...NursingISBN:9780323414425Author:Robert J Hubert BSPublisher:Saunders Fundamentals Of NursingNursingISBN:9781496362179Author:Taylor, Carol (carol R.), LYNN, Pamela (pamela Barbara), Bartlett, Jennifer L.Publisher:Wolters Kluwer,
Fundamentals Of NursingNursingISBN:9781496362179Author:Taylor, Carol (carol R.), LYNN, Pamela (pamela Barbara), Bartlett, Jennifer L.Publisher:Wolters Kluwer,  Fundamentals of Nursing, 9eNursingISBN:9780323327404Author:Patricia A. Potter RN MSN PhD FAAN, Anne Griffin Perry RN EdD FAAN, Patricia Stockert RN BSN MS PhD, Amy Hall RN BSN MS PhD CNEPublisher:Elsevier Science
Fundamentals of Nursing, 9eNursingISBN:9780323327404Author:Patricia A. Potter RN MSN PhD FAAN, Anne Griffin Perry RN EdD FAAN, Patricia Stockert RN BSN MS PhD, Amy Hall RN BSN MS PhD CNEPublisher:Elsevier Science Study Guide for Gould's Pathophysiology for the H...NursingISBN:9780323414142Author:Hubert BS, Robert J; VanMeter PhD, Karin C.Publisher:Saunders
Study Guide for Gould's Pathophysiology for the H...NursingISBN:9780323414142Author:Hubert BS, Robert J; VanMeter PhD, Karin C.Publisher:Saunders Issues and Ethics in the Helping Professions (Min...NursingISBN:9781337406291Author:Gerald Corey, Marianne Schneider Corey, Cindy CoreyPublisher:Cengage Learning
Issues and Ethics in the Helping Professions (Min...NursingISBN:9781337406291Author:Gerald Corey, Marianne Schneider Corey, Cindy CoreyPublisher:Cengage Learning
Phlebotomy Essentials
Nursing
ISBN:9781451194524
Author:Ruth McCall, Cathee M. Tankersley MT(ASCP)
Publisher:JONES+BARTLETT PUBLISHERS, INC.
Gould's Pathophysiology for the Health Profession...
Nursing
ISBN:9780323414425
Author:Robert J Hubert BS
Publisher:Saunders
Fundamentals Of Nursing
Nursing
ISBN:9781496362179
Author:Taylor, Carol (carol R.), LYNN, Pamela (pamela Barbara), Bartlett, Jennifer L.
Publisher:Wolters Kluwer,
Fundamentals of Nursing, 9e
Nursing
ISBN:9780323327404
Author:Patricia A. Potter RN MSN PhD FAAN, Anne Griffin Perry RN EdD FAAN, Patricia Stockert RN BSN MS PhD, Amy Hall RN BSN MS PhD CNE
Publisher:Elsevier Science
Study Guide for Gould's Pathophysiology for the H...
Nursing
ISBN:9780323414142
Author:Hubert BS, Robert J; VanMeter PhD, Karin C.
Publisher:Saunders
Issues and Ethics in the Helping Professions (Min...
Nursing
ISBN:9781337406291
Author:Gerald Corey, Marianne Schneider Corey, Cindy Corey
Publisher:Cengage Learning