NATIONAL CENTER FOR CASE STUDY TEACHING IN SCIENCE Normal ventricular pressure values: Right ventricle: 25mmHg systolic; 4mmHg diastolic Left ventricle: 120mmHg systolic, 10 mmHg diastolic iii. Would enough oxygenated blood enter the systemic circuit? Explain. iv. Use an arrow to indicate on the flowchart used in Question 5 above where VSD would occur. v. Pavit presents with severe pulmonary hypertension; explain how VSD can lead to this. vi. Indicate on the heart diagram to the right where VSD would be present:
NATIONAL CENTER FOR CASE STUDY TEACHING IN SCIENCE Normal ventricular pressure values: Right ventricle: 25mmHg systolic; 4mmHg diastolic Left ventricle: 120mmHg systolic, 10 mmHg diastolic iii. Would enough oxygenated blood enter the systemic circuit? Explain. iv. Use an arrow to indicate on the flowchart used in Question 5 above where VSD would occur. v. Pavit presents with severe pulmonary hypertension; explain how VSD can lead to this. vi. Indicate on the heart diagram to the right where VSD would be present:

Phlebotomy Essentials
6th Edition
ISBN:9781451194524
Author:Ruth McCall, Cathee M. Tankersley MT(ASCP)
Publisher:Ruth McCall, Cathee M. Tankersley MT(ASCP)
Chapter1: Phlebotomy: Past And Present And The Healthcare Setting
Section: Chapter Questions
Problem 1SRQ

Related questions
Question
Transcribed Image Text:NATIONAL CENTER FOR CASE STUDY TEACHING IN SCIENCE
Normal ventricular pressure values:
Right ventricle: 25mmHg systolic; 4mmHg diastolic
Left ventricle: 120mmHg systolic, 10 mmHg diastolic
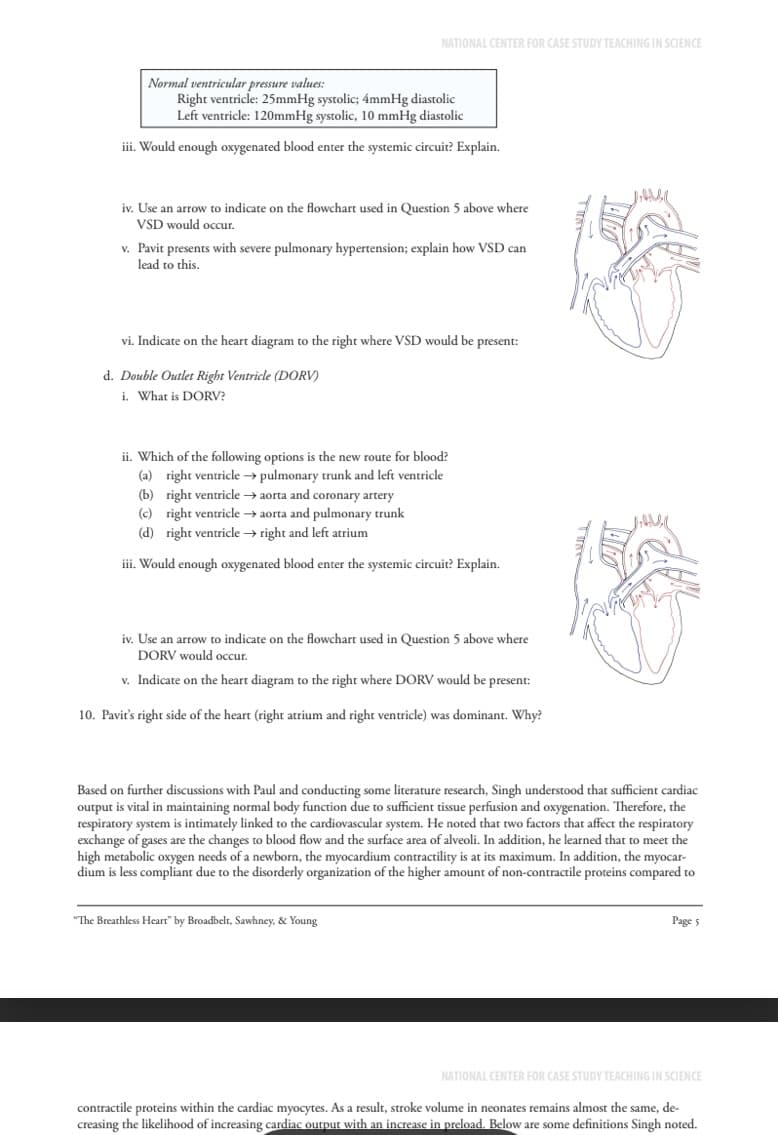
iii. Would enough oxygenated blood enter the systemic circuit? Explain.
iv. Use an arrow to indicate on the flowchart used in Question 5 above where
VSD would occur.
v. Pavit presents with severe pulmonary hypertension; explain how VSD can
lead to this.
vi. Indicate on the heart diagram to the right where VSD would be present:
d. Double Outlet Right Ventricle (DORV)
i. What is DORV?
ii. Which of the following options is the new route for blood?
(a) right ventricle → pulmonary trunk and left ventricle
(b) right ventricle→aorta and coronary artery
(c) right ventricle → aorta and pulmonary trunk
(d) right ventricle → right and left atrium
iii. Would enough oxygenated blood enter the systemic circuit? Explain.
iv. Use an arrow to indicate on the flowchart used in Question 5 above where
DORV would occur.
v. Indicate on the heart diagram to the right where DORV would be present:
10. Pavir's right side of the heart (right atrium and right ventricle) was dominant. Why?
Based on further discussions with Paul and conducting some literature research, Singh understood that sufficient cardiac
output is vital in maintaining normal body function due to sufficient tissue perfusion and oxygenation. Therefore, the
respiratory system is intimately linked to the cardiovascular system. He noted that two factors that affect the respiratory
exchange of gases are the changes to blood flow and the surface area of alveoli. In addition, he learned that to meet the
high metabolic oxygen needs of a newborn, the myocardium contractility is at its maximum. In addition, the myocar-
dium is less compliant due to the disorderly organization of the higher amount of non-contractile proteins compared to
"The Breathless Heart" by Broadbelt, Sawhney, & Young
Page 5
NATIONAL CENTER FOR CASE STUDY TEACHING IN SCIENCE
contractile proteins within the cardiac myocytes. As a result, stroke volume in neonates remains almost the same, de-
creasing the likelihood of increasing cardiac output with an increase in preload. Below are some definitions Singh noted.
Transcribed Image Text:NATIONAL CENTER FOR CASE STUDY TEACHING IN SCIENCE
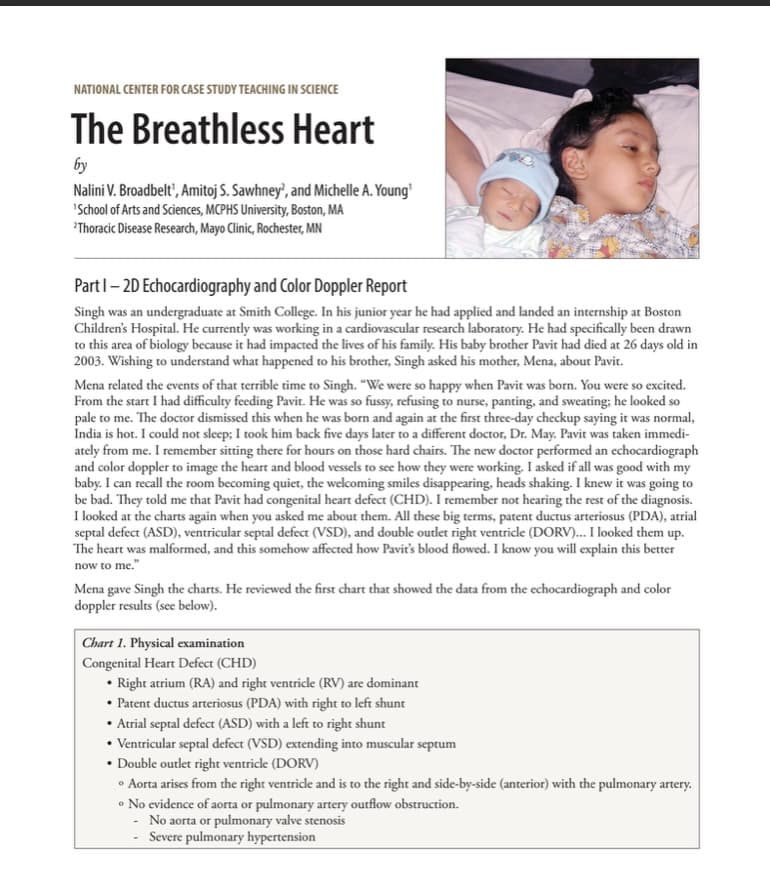
The Breathless Heart
by
Nalini V. Broadbelt', Amitoj S. Sawhney?, and Michelle A. Young'
'School of Arts and Sciences, MCPHS University, Boston, MA
Thoracic Disease Research, Mayo Clinic, Rochester, MN
Part 1-2D Echocardiography and Color Doppler Report
Singh was an undergraduate at Smith College. In his junior year he had applied and landed an internship at Boston
Children's Hospital. He currently was working in a cardiovascular research laboratory. He had specifically been drawn
to this area of biology because it had impacted the lives of his family. His baby brother Pavit had died at 26 days old in
2003. Wishing to understand what happened to his brother, Singh asked his mother, Mena, about Pavit.
Mena related the events of that terrible time to Singh. "We were so happy when Pavit was born. You were so excited.
From the start I had difficulty feeding Pavit. He was so fussy, refusing to nurse, panting, and sweating; he looked so
pale to me. The doctor dismissed this when he was born and again at the first three-day checkup saying it was normal,
India is hot. I could not sleep; I took him back five days later to a different doctor, Dr. May. Pavit was taken immedi-
ately from me. I remember sitting there for hours on those hard chairs. The new doctor performed an echocardiograph
and color doppler to image the heart and blood vessels to see how they were working. I asked if all was good with my
baby. I can recall the room becoming quiet, the welcoming smiles disappearing, heads shaking. I knew it was going to
be bad. They told me that Pavit had congenital heart defect (CHD). I remember not hearing the rest of the diagnosis.
I looked at the charts again when you asked me about them. All these big terms, patent ductus arteriosus (PDA), atrial
septal defect (ASD), ventricular septal defect (VSD), and double outlet right ventricle (DORV)... I looked them up.
The heart was malformed, and this somehow affected how Pavit's blood flowed. I know you will explain this better
now to me."
Mena gave Singh the charts. He reviewed the first chart that showed the data from the echocardiograph and color
doppler results (see below).
Chart 1. Physical examination
Congenital Heart Defect (CHD)
• Right atrium (RA) and right ventricle (RV) are dominant
⚫ Patent ductus arteriosus (PDA) with right to left shunt
⚫ Atrial septal defect (ASD) with a left to right shunt
• Ventricular septal defect (VSD) extending into muscular septum
⚫ Double outlet right ventricle (DORV)
• Aorta arises from the right ventricle and is to the right and side-by-side (anterior) with the pulmonary artery.
• No evidence of aorta or pulmonary artery outflow obstruction.
-No aorta or pulmonary valve stenosis
Severe pulmonary hypertension
Expert Solution
This question has been solved!
Explore an expertly crafted, step-by-step solution for a thorough understanding of key concepts.

This is a popular solution!

Trending now
This is a popular solution!

Step by step
Solved in 5 steps with 1 images

Follow-up Questions
Read through expert solutions to related follow-up questions below.
Follow-up Question
Answer all questions starting from what is DORV

Transcribed Image Text:Superior and
Inferior venae
cavae
REST OF
THE BODY
Right
Atrium
Tricuspid
valve
Coronary veins
L
Right ventricle
and sinus
HEART
L
Coronary
arteries
Aorta
Aortic
semilunar
valves
Left ventricle
Pulmonary
semilunar
valve
Pulmonary
trunk
Bicuspid
valve
Left atrium
Pulmonary
arteries
LUNG
Pulmonary
veins

Transcribed Image Text:NATIONAL CENTER FOR CASE STUDY TEACHING IN SCIENCE
Normal ventricular pressure values:
Right ventricle: 25mmHg systolic; 4mmHg diastolic
Left ventricle: 120mmHg systolic, 10 mmHg diastolic
iii. Would enough oxygenated blood enter the systemic circuit? Explain.
iv. Use an arrow to indicate on the flowchart used in Question 5 above where
VSD would occur.
v. Pavit presents with severe pulmonary hypertension; explain how VSD can
lead to this.
vi. Indicate on the heart diagram to the right where VSD would be present:
d. Double Outlet Right Ventricle (DORV)
i. What is DORV?
ii. Which of the following options is the new route for blood?
(a) right ventricle → pulmonary trunk and left ventricle
(b) right ventricle→aorta and coronary artery
(c) right ventricle → aorta and pulmonary trunk
(d) right ventricle → right and left atrium
iii. Would enough oxygenated blood enter the systemic circuit? Explain.
iv. Use an arrow to indicate on the flowchart used in Question 5 above where
DORV would occur.
v. Indicate on the heart diagram to the right where DORV would be present:
10. Pavir's right side of the heart (right atrium and right ventricle) was dominant. Why?
Based on further discussions with Paul and conducting some literature research, Singh understood that sufficient cardiac
output is vital in maintaining normal body function due to sufficient tissue perfusion and oxygenation. Therefore, the
respiratory system is intimately linked to the cardiovascular system. He noted that two factors that affect the respiratory
exchange of gases are the changes to blood flow and the surface area of alveoli. In addition, he learned that to meet the
high metabolic oxygen needs of a newborn, the myocardium contractility is at its maximum. In addition, the myocar-
dium is less compliant due to the disorderly organization of the higher amount of non-contractile proteins compared to
"The Breathless Heart" by Broadbelt, Sawhney, & Young
Page 5
NATIONAL CENTER FOR CASE STUDY TEACHING IN SCIENCE
contractile proteins within the cardiac myocytes. As a result, stroke volume in neonates remains almost the same, de-
creasing the likelihood of increasing cardiac output with an increase in preload. Below are some definitions Singh noted.
Solution
Recommended textbooks for you
Phlebotomy Essentials
Nursing
ISBN:
9781451194524
Author:
Ruth McCall, Cathee M. Tankersley MT(ASCP)
Publisher:
JONES+BARTLETT PUBLISHERS, INC.

Gould's Pathophysiology for the Health Profession…
Nursing
ISBN:
9780323414425
Author:
Robert J Hubert BS
Publisher:
Saunders

Fundamentals Of Nursing
Nursing
ISBN:
9781496362179
Author:
Taylor, Carol (carol R.), LYNN, Pamela (pamela Barbara), Bartlett, Jennifer L.
Publisher:
Wolters Kluwer,
Phlebotomy Essentials
Nursing
ISBN:
9781451194524
Author:
Ruth McCall, Cathee M. Tankersley MT(ASCP)
Publisher:
JONES+BARTLETT PUBLISHERS, INC.
Gould's Pathophysiology for the Health Profession…
Nursing
ISBN:
9780323414425
Author:
Robert J Hubert BS
Publisher:
Saunders
Fundamentals Of Nursing
Nursing
ISBN:
9781496362179
Author:
Taylor, Carol (carol R.), LYNN, Pamela (pamela Barbara), Bartlett, Jennifer L.
Publisher:
Wolters Kluwer,

Fundamentals of Nursing, 9e
Nursing
ISBN:
9780323327404
Author:
Patricia A. Potter RN MSN PhD FAAN, Anne Griffin Perry RN EdD FAAN, Patricia Stockert RN BSN MS PhD, Amy Hall RN BSN MS PhD CNE
Publisher:
Elsevier Science

Study Guide for Gould's Pathophysiology for the H…
Nursing
ISBN:
9780323414142
Author:
Hubert BS, Robert J; VanMeter PhD, Karin C.
Publisher:
Saunders

Issues and Ethics in the Helping Professions (Min…
Nursing
ISBN:
9781337406291
Author:
Gerald Corey, Marianne Schneider Corey, Cindy Corey
Publisher:
Cengage Learning